Ο καρκίνος του μαστού
Ο καρκίνος του μαστού συμβαίνει συχνά στις γυναίκες, μια στις 10, και πολύ σπάνια στους άνδρες. Ωστόσο, με την έγκαιρη διάγνωση έχει και πολύ καλή πρόγνωση, μιας και το 90% των γυναικών που θα συμβεί δεν θα έχουν κανένα πρόβλημα στο μέλλον. Προϋπόθεση,βέβαια, για την καλύτερη έκβαση είναι: η έγκαιρη διάγνωση και η σωστή αντιμετώπιση.
Η έγκαιρη διάγνωση είναι αποτέλεσμα της σωστής πληροφόρησης για σημάδια ύπαρξης του καρκίνου, της σωστής παρακολούθησης και της χρήσης της κατάλληλης διαγνωστικής μεθόδου.
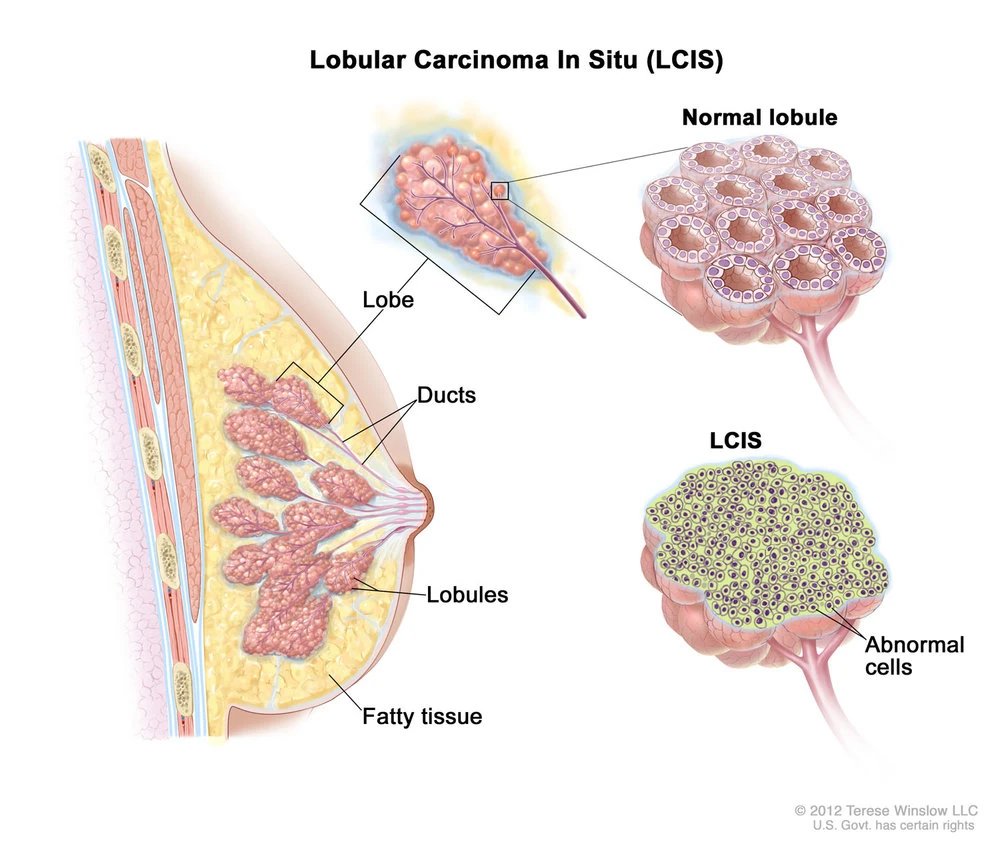
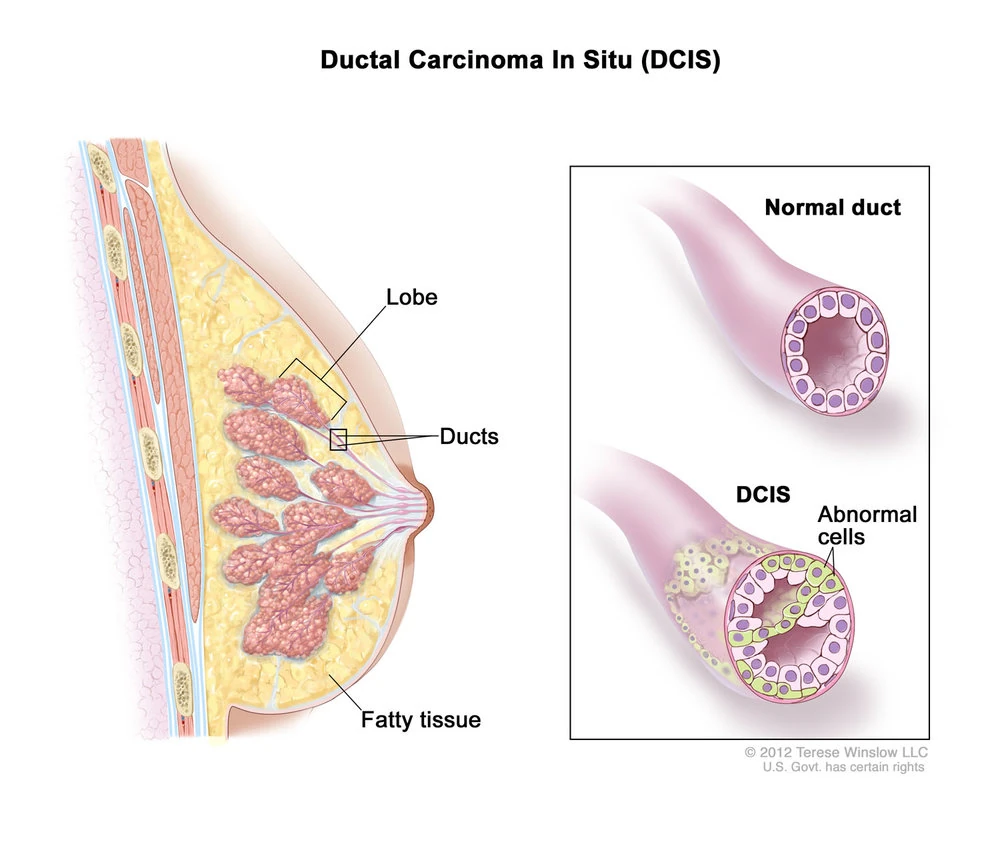
Προκαρκινικές βλάβες των μαστών που διαγιγνώσκονται κυρίως με τον προληπτικό έλεγχο
Ο καρκίνος του μαστού
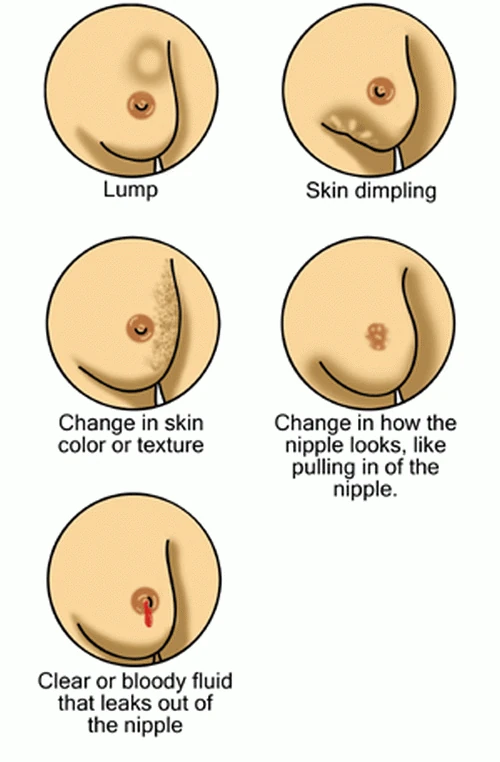
Τα σημάδια ύπαρξης καρκίνου μαστού
Τα σημάδια ύπαρξης καρκίνου μαστού είναι η ύπαρξη ογκιδίου στο μαστό ή τη μασχάλη, η παραμόρφωση του μαστού, η εισολκή του δέρματος, το αιματηρό έκκριμα της θηλής και η φλεγμονή.
Κάποιες προηγούμενες βιοψίες με προκαρκινικές βλάβες οδηγούν σε πιο συχνό έλεγχο.

Εισολκή θηλής

Στάδια Καρκίνου Μαστού
Ανάλογα με το μέγεθος του όγκου, την διήθηση των λεμφαδένων και τις μεταστάσεις
Ο καρκίνος του μαστού
Διαγνωστική μέθοδος
Η σωστή παρακολούθηση των μαστών γίνεται με τον τρόπο και τη συχνότητα που θα καθορίσει ο χειρουργός μαστού.
Τα κριτήρια στα οποία βασίζεται η επιλογή είναι η ύπαρξη παραγόντων κινδύνου, η ηλικία των γυναικών, η σύσταση των μαστών, τα ευρήματα των προηγουμένων εξετάσεων και ορισμένες προηγούμενες βιοψίες.
Ο κυριότερος παράγων κινδύνου είναι η κληρονομικότητα και όσο πιο ισχυρός είναι τόσο πιο σε μικρότερη ηλικία, πιο συχνά και με περισσότερες εξετάσεις πρέπει να γίνεται ο έλεγχος.
Η μικρότερη ηλικία και η μεγάλη πυκνότητα των μαστών σημαίνουν και τη χρήση εκτός της μαστογραφίας και του υπερηχογραφήματος και της μαγνητικής μαστογραφίας στον έλεγχο. Κάποιες προηγούμενες βιοψίες με προκαρκινικές βλάβες οδηγούν σε πιο συχνό έλεγχο.
Η κατάλληλη διαγνωστική μέθοδος, στην περίπτωση που διαπιστωθεί στις εξετάσεις ελέγχου κάποια βλάβη, αποτελεί επιλογή του χειρουργού μαστού στο εξωτερικό ιατρείο μεταξύ παρακέντησης με λεπτή βελόνη και εξέταση (FNA), βιοψία με κόπτουσα βελόνα (Core biopsy) mammotome ή BLES και ιστολογική εξέταση και ανοικτή βιοψία στο χειρουργείο. Πρέπει σε όλες τις περιπτώσεις που είναι δυνατόν, να έχουμε ιστολογική διάγνωση πριν την χειρουργική επέμβαση.
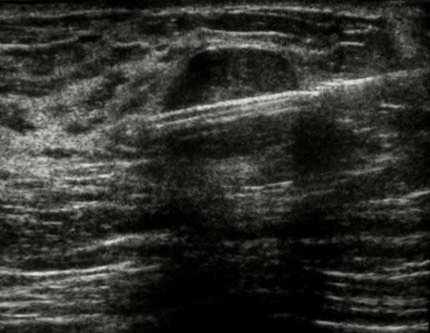
Βιοψία με κόπτουσα βελόνη με τη βοήθεια υπερηχογράφου

Βιοψία με κόπτουσα βελόνη με τη βοήθεια υπερηχογράφου

Βιοψία με συρμάτινο οδηγό για περιπτώσεις που η βλάβη του μαστού δεν είναι ψηλαφητή.

Η μαστογραφική απεικόνιση του συρμάτινου οδηγού.

Αριστερά ο συρμάτινος οδηγός μέσα στη βλάβη – μαστογραφία. Δεξιά μετά την αφαίρεση της βλάβης γίνεται μαστογραφία του ιστού που αφαιρέθηκε για να πιστοποιηθεί η σωστή αφαίρεση.
Ο καρκίνος του μαστού
Αντιμετώπιση
Η σωστή αντιμετώπιση αποτελεί ευθύνη του χειρουργού μαστού ο οποίος σε συνεργασία με την κατάλληλη ομάδα ειδικευμένων στο καρκίνο του μαστού ακτινολόγων, ογκολόγων, ακτινοθεραπευτών και ενδεχομένως πλαστικών χειρουργών στα πλαίσια συμβουλίου, θα αποφασίσει για την κατάλληλη θεραπεία. Στην θεραπεία του καρκίνου του μαστού περιλαμβάνονται ανάλογα με την περίπτωση προεγχειρητική θεραπεία, χειρουργική επέμβαση και συμπληρωματικής θεραπείας με χημειοθεραπεία, ορμονοθεραπεία και ακτινοθεραπεία.

Bιοψία φρουρού λεφαδένα. Στη περίπτωση που οι λεμφαδένες της μασχάλης δεν είναι ύποπτοι στη ψηλάφηση και στο υπερηχογράφημα πρέπει να γίνει βιοψία φρουρού λεφαδένα με έγχυση ραδιοϊσοτόπου λίγες ώρες πριν και κυανού του μεθυλενίου άμεσα πριν την χειρουργική επέμβαση.

Ο φρουρός λεμφαδένας όπως φαίνεται στη επέμβαση.

Ο ανιχνευτής γ-ακτινοβολίας που χρησιμοποιείται στο χειρουργείο για να εντοπίσουμε τον φρουρό λεμφαδένα που το ραδιοϊσότοπο έχει πάει.

Το άμεσο μετεγχειρητικό αποτέλεσμα μετά αφαίρεση ογκιδίου μαστού και βιοψία φρουρού λεμφαδένα. Έχει αποφευχθεί ο λεμφαδενικός καθαρισμός που συχνά προκαλεί άλγος και λεμφοίδημα.
“Η επιστήμη εξελίσσεται γρήγορα και μπορεί αυτά που λέμε σήμερα σε λίγες μέρες να αλλάξουν. Δεν πρέπει λοιπόν να θεωρούμε δεδομένο και σταθερό κάθε τι που διαβάζουμε. Η συζήτηση με τον ειδικό, που έχει καθήκον να ενημερώνεται καθημερινά, δεν μπορεί να αντικατασταθεί από κανένα κείμενο. ”